
About Microtia
What is microtia?
Microtia (my-KRO-sha) is the incomplete development and growth of the outer ear. This can lead to a small, abnormally shaped or absent ear. It usually involves one side, though both ears may be affected in some children.
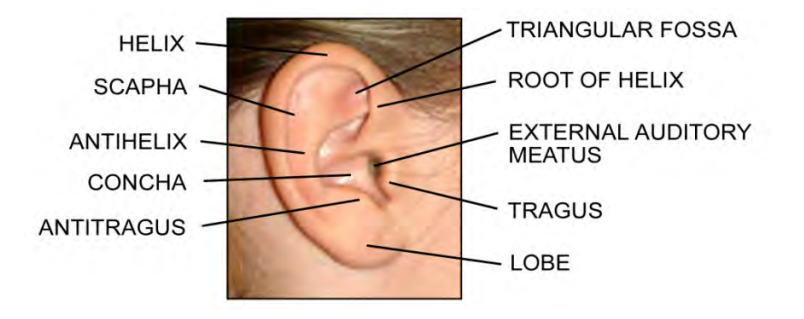
Typical ear anatomy
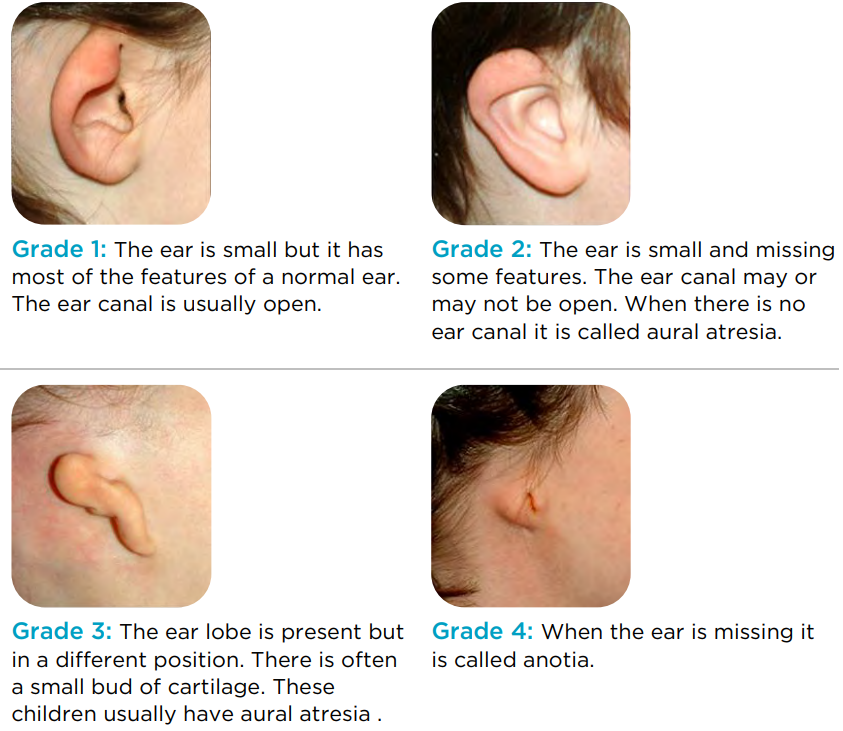
Microtia can be divided into four types:
Frequently Asked Questions
+ Will my child have other problems related to the microtia?
Many children with microtia also have a small jaw on the same side. This is called hemifacial microsomia (HFM) or craniofacial microsomia (CFM). Many children with microtia also have mild abnormalities of their normal ear. About 10% of children with microtia have abnormalities in other systems. These may include facial clefts, heart defects, eye, kidney and spine (vertebral) abnormalities.
+ Why does my child have microtia?
Most of the time we do not know what caused the ear to form abnormally. Exposure to high doses of vitamin A and maternal diabetes during pregnancy are two of the known causes of microtia. There are also some syndromes associated with small ears. These include: Treacher-Collins syndrome, oculoauriculovertebral (ah-CUE-lo-aw-RICK-oh-lo-ver-TEE-bral) syndrome and Goldenhar syndrome. Microtia may run in your family. A specific gene has not been identified yet. Right now, there are no tests to show the cause of microtia.
+ What should we do for our child?
Start by having your child’s hearing tested. We expect that your child will have some hearing loss in the small ear. The hearing test will also tell us about the hearing in the other ear. Children with normal hearing in one ear often develop normal speech and language. However, the presence of hearing loss in one ear can also present some challenges for young children as they learn speech and language.
There are two main types of hearing tests: BAER (brainstem auditory evoked responses) and behavioral testing (audiogram). BAER testing is performed if your child is too young to cooperate with behavioral testing. Behavioral testing is done when the child is mature enough to cooperate. Other tests may be recommended, based on your child’s age. Based upon the results of the hearing tests, the audiologist and otolaryngologist will discuss the options for hearing management.
Care Recommendations by Age
+ Infancy (0-12 months)
• Routine well-child care (including assessment of heart and kidneys)
• Hearing evaluation
• Hearing loss intervention if needed
• Renal (kidney) ultrasound
• Consider band-retained bone conduction sound processor
+ Toddlers (1-3 years old)
• Routine well-child care
• Hearing evaluation
• Consider band retained bone conduction sound processor
• Consider a speech and language evaluation
+ Preschool (3-5 years old)
• Routine well-child care
• Hearing evaluation
• Consider band retained bone conduction sound processor
• Consider a speech and language evaluation
• Dental assessment
+ Early school (5-7 years old)
• Routine well-child care
• Hearing evaluation
• Consider speech and language evaluation
• Dental assessment
• Review options for microtia management
• CT scan of the temporal bones (for children with hearing loss)
• Review options for hearing management
• Neck X-rays
• School accommodations, as needed
+ School age (7-9 years)
• Consider ear reconstruction
• Consider options for hearing management
• Evaluate jaw symmetry
This information was provided by the Seattle Children’s Craniofacial Care Team. More information can be found here.